The text you provided outlines standard medical advice regarding Polycystic Ovary Syndrome (PCOS) and contraceptive management. However, when we look at endocrine disorders, simply listing “the pill or the patch” does not explain the biological mechanisms at play. If you want to successfully manage PCOS, you must understand the exact hormonal mathematics that are driving your symptoms.
PCOS is fundamentally a disorder of hyperandrogenism and insulin resistance. The reason hormonal birth control is considered a first-line therapy is not just for contraception; it is a targeted biochemical intervention designed to suppress the massive overproduction of ovarian androgens. Here is the clinical reality of how these methods mathematically and biologically alter your endocrine system.
The Biological Reality: The LH/FSH Ratio and Androgen Suppression
In a biologically typical menstrual cycle, the pituitary gland releases Follicle-Stimulating Hormone (FSH) and Luteinizing Hormone (LH) in a highly regulated sequence. In a patient with PCOS, this ratio is broken.
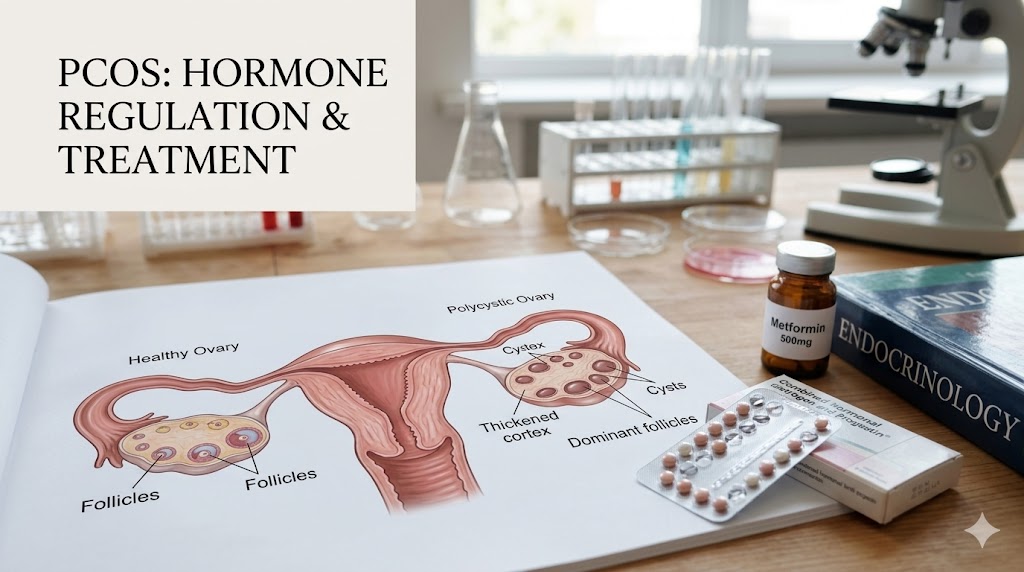
Patients with PCOS frequently present with an elevated LH/FSH ratio. The massive surge of LH forces the theca cells in the ovaries to aggressively overproduce androgens (specifically testosterone and androstenedione). These androgens are what cause the visible symptoms: severe cystic acne, hirsutism (excess facial and body hair), and male-pattern baldness.
The Mechanism of Action (Estrogen and Progestin)
When you introduce a combined oral contraceptive (containing synthetic estrogen and progestin), you introduce negative feedback to the pituitary gland.
- The synthetic hormones suppress the release of GnRH (Gonadotropin-Releasing Hormone) from the hypothalamus.
- This stops the pituitary from releasing the massive, erratic surges of LH.
- Without the LH surge, the ovaries are no longer stimulated to pump out excess testosterone.
Furthermore, the synthetic estrogen in the pill drastically increases the liver’s production of Sex Hormone-Binding Globulin (SHBG). SHBG acts like a biological sponge, binding up the free, floating testosterone in your blood so it cannot attach to your hair follicles or sebaceous glands.
02. Endometrial Protection: The Mathematics of Cancer Risk
One of the most dangerous, silent aspects of PCOS is oligo-ovulation (infrequent ovulation). When you do not ovulate, your body does not produce progesterone.
Without the opposing force of progesterone, the continuous, unopposed estrogen causes the endometrial lining to thicken indefinitely. This creates a severe risk for endometrial hyperplasia and, eventually, endometrial cancer. Clinical data indicates that women with PCOS are up to 2.7 times more likely to develop endometrial cancer.
By introducing synthetic progestin via a daily pill, a patch, or an intrauterine device (IUD), you physically force the endometrial lining to shed or remain safely thin. We can look at the risk reduction mathematically:
$$Risk_{cancer} = BaseRisk \times e^{-k \cdot (Duration_{BC})}$$
Where continuous exposure to synthetic progestin ($Duration_{BC}$) exponentially decreases ($e^{-k}$) the risk of malignant cellular mutation by nearly 30% over time.
Navigating the Progestin Variables
Not all birth control is created equal for PCOS. The type of synthetic progestin used in the formulation is the critical variable. Some older generation progestins are highly androgenic, meaning they act like testosterone in the body, which will actually make your PCOS symptoms (like acne and hair growth) worse.
When consulting with your physician or utilizing telehealth platforms like Nurx or SimpleHealth, you must explicitly request a combination pill containing a low-androgenic or anti-androgenic progestin.
Anti-Androgenic Progestins (Ideal for PCOS):
- Drospirenone (Found in Yaz, Yasmin)
- Norgestimate (Found in Ortho Tri-Cyclen)
- Desogestrel
Avoid pills containing Levonorgestrel or Norgestrel if your primary goal is to clear severe acne or hirsutism, as these possess higher androgenic activity.
The Cardiometabolic Warning
While birth control is highly effective for symptom management, it does not cure the underlying metabolic dysfunction of PCOS. Many patients with PCOS suffer from severe insulin resistance.
Taking oral contraceptives, particularly those containing estrogen, can slightly elevate blood pressure and increase the risk of venous thromboembolism (blood clots). If a patient with PCOS is also obese, a heavy smoker, or over the age of 35, the cardiometabolic risks of the estrogen pill may outweigh the benefits. In these specific cases, a localized progestin-only method, such as a Mirena IUD, is often the safest clinical choice to protect the endometrium without risking systemic cardiovascular events.best birth control for pcos
Conclusion
For patients battling PCOS, hormonal birth control is not merely a contraceptive; it is a highly calculated endocrine intervention. By suppressing LH production, binding free testosterone with SHBG, and chemically protecting the uterine lining with targeted progestins, these medications alter the biological landscape of the disorder. However, success depends entirely on selecting the correct generation of progestin and continuously monitoring the cardiometabolic risks alongside your physician.